Skaphe (boat) + cephalus (head)
& Dolikhos (long) + cephalus (head)
Scaphocephaly/Dolichocephaly are descriptive terms for a skull that is abnormally longer than it is wide, with a cephalic index <75 for women and < 75.9 for men. Scaphocephaly/Dolichocephaly is the most common kind of
simple craniosynostosis, comprising 40-55% of nonsyndromic cases. Craniosynostoses occur with a frequency of 1:2000-2500.
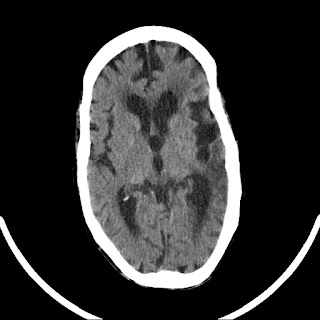 |
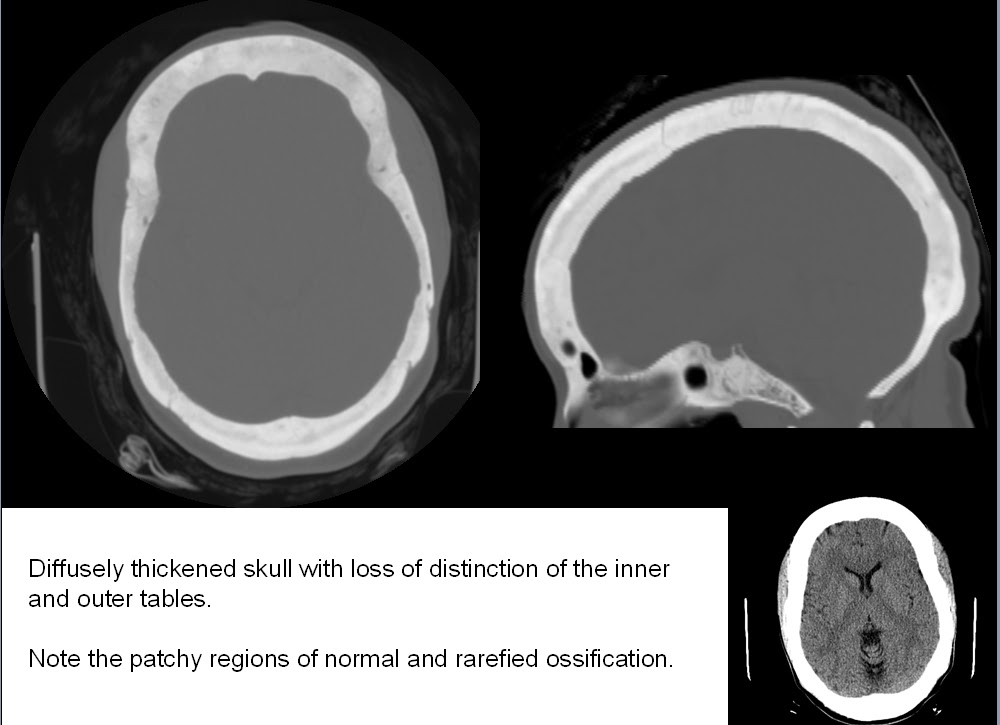
Scaphocephalic/Dolichocephalic skull
(old left MCA infarct as well) |
 |
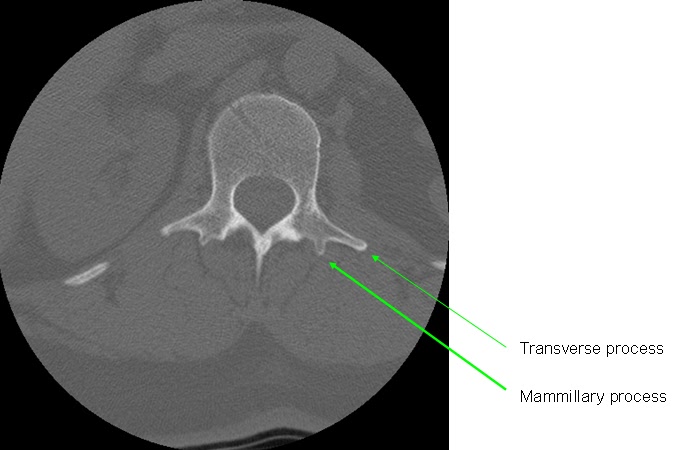
| Scout radiograph of same patient |
The
cephalic index was originally devised by Anders Retzius (the same with the "space" named after him). It's simply a ratio of the widest AP and TV distances of the skull. (The TV distance is the same as the biparietal diameter, BPD). Virchow (the same with the "triad" named after him) pointed out that when a suture closes prematurely (in scaphocephaly, the sagittal), then the growth of the skull is restricted in the plane
perpendicular to the suture, and compensate in the parallel direction.
The scaphocephaly demonstrated above is a
simple form of craniosynostosis... simple in the sense that only one suture has prematurely fused, the sagittal. Other simple craniosynostosis include
brachycephaly (premature fusion of the coronal suture) and
trigonocephaly ("keel skull," premature fusion of the metopic suture).
Compound craniosynostosis involves more than one suture, such as in
plagiocephaly ("skew skull").
Although certainly a morphologic/aesthetic issue, and frequently related to congenital syndromes, the craniosynostoses may also occur by themselves and have no other associated effects. One source mentions that the formation of craniosynostoses may have an effect on the underlying CSF spaces -- decreased/eliminated at the premature suture line, excessive in the areas of abnormally increased skull space
The concept of "appropriate" skull size is species-specific, since some animals are
supposed to have skulls longer than they are wide... and you could just as easily call scaphocephaly "greyhound skull" since the greyhound is one of the many dogs whose heads are normally scaphocephalic:
 |
| The greyhound: a normally scaphocephalic dog |
Although the two terms
scaphocephaly and
dolichocephaly are synonymous, the term
dolichocephaly may be a more consistent fit with the other end of the spectrum,
brachycephaly ("short skull"). Incidentally, between the two lies the more or less useless term
mesaticephaly.
-----
1. Benson ML, Oliverio PJ, Yue NC, Zinreich SJ. Primary Craniosynostosis: Imaging Features. AJR 1996;166:697-703 036
2. Delashaw JB, et al. Cranial Vault Growth in Synostosis: Review Article. JNS 70:159-165, 1989